
Non-Surgical Treatment for Knee Osteoarthritis
- Emma Glynn
- Jun 15
- 10 min read

By Emma Glynn - The Hip & Knee Physio
If you have been told you have knee osteoarthritis, it is understandable if your mind jumps straight to surgery. Many people hear phrases like “bone on bone”, “degenerative change”, or “you will need a knee replacement one day”, then leave the appointment wondering whether there is anything useful to do now.
There usually is...

Non-surgical treatment for knee osteoarthritis is not about pretending the joint has no changes; it is about improving what the knee can tolerate, reducing flare cycles, and helping you stay active for as long as possible.
The strongest evidence for knee OA management consistently points toward education, exercise, physical activity, and weight management where relevant (Australian Commission on Safety and Quality in Health Care, 2024; Bannuru et al., 2019; Kolasinski et al., 2020). Surgery can be very helpful for some people, but for many, it is not the first step.
I am Emma Glynn, an APA Titled Musculoskeletal Physiotherapist in Camberwell. I work exclusively with hip and knee conditions, and I often assess active adults over 45 who have been told they have knee arthritis but have not been given a clear plan.
For a broader overview of the condition, you can visit my knee osteoarthritis page.
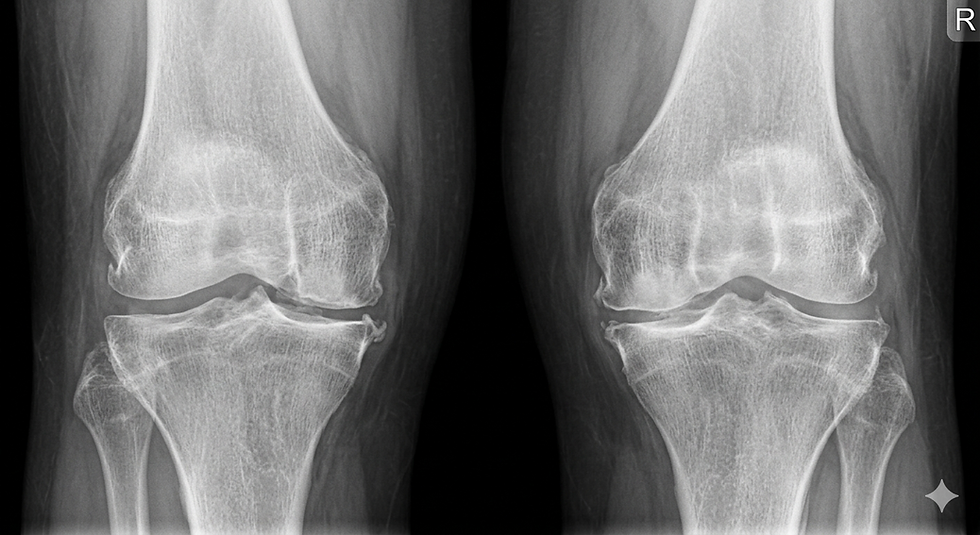
Why bone on bone does not automatically mean surgery
“Bone on bone” is one of the most alarming phrases people hear about knee arthritis. It usually refers to significant joint space narrowing on an X-ray, often because there is advanced cartilage loss in one part of the knee.
That matters, but it does not tell the whole story.
The X-ray can describe joint changes, but it does not fully explain your pain, strength, walking tolerance, confidence, or treatment options.
Research has consistently shown a mismatch between X-ray findings and symptoms in knee OA. Some people have significant radiographic changes with manageable pain. Others have mild X-ray changes but significant symptoms and functional limitation (Bedson & Croft, 2008; Finan et al., 2013).
A useful assessment looks at more than imaging. It considers:
What activities trigger your pain
Whether your symptoms flare and settle
How strong your quadriceps and hip muscles are
Whether swelling is limiting movement
How you manage stairs, hills, squats or low chairs
What you want to get back to
Whether another diagnosis needs to be considered
If you are still trying to work out whether your symptoms fit knee OA, start with this guide to knee arthritis symptoms and early signs of knee osteoarthritis.
Non-surgical treatment for knee osteoarthritis starts with education
Education sounds boring, but it is one of the most important parts of knee OA care. Not fluffy reassurance. Not “just keep moving”. Proper education should help you understand what OA is, what it is not, what drives flare-ups, and how to make better decisions with activity.
People manage knee OA better when they understand that pain does not always equal damage, and that the right amount of movement is usually helpful.
Good education should cover:
Why knee OA is a whole-joint condition, not just “worn cartilage”
Why symptoms can vary from day to day
How to recognise a flare-up
How to modify activity without stopping everything
Why strength matters
When pain during exercise is acceptable and when it is a warning sign
When medical review or imaging may be appropriate
This matters because many people get stuck in a boom-bust cycle. They rest until the knee feels better, do too much on a good day, flare for several days, then rest again. A clearer understanding of load can help break that cycle.
Exercise is the cornerstone of non-surgical treatment for knee osteoarthritis
Exercise therapy is one of the most consistently recommended treatments for knee OA. The goal is not to punish the joint or force through severe pain. The goal is to build strength, confidence and load tolerance in a way the knee can handle.
The best exercise program is not the hardest program; it is the one your knee can tolerate, repeat and gradually progress.
A Cochrane review found that land-based exercise can reduce pain and improve function in people with knee OA (Fransen et al., 2015). A 2025 BMJ network meta-analysis also found that different exercise types can improve pain, function, gait performance and quality of life, with aerobic exercise ranking highly across several outcomes (Yan et al., 2025).
For knee OA, exercise may include:
Strength training: especially quadriceps, hip, calf and trunk strengthening
Aerobic activity: walking, cycling, swimming or other options matched to your tolerance
Neuromuscular training: improving balance, control, stepping, landing and direction changes
Mobility work: maintaining comfortable movement without forcing painful ranges
Functional training: sit-to-stand, stairs, step-ups, squats or loaded carries
The entry point matters. A person who flares after ten minutes of walking does not need the same plan as someone who wants to keep running 10 kilometres.
If you are wondering about running specifically, I have written more here: Can you keep running with knee osteoarthritis?
Physiotherapy for knee osteoarthritis should be specific
Physiotherapy for knee osteoarthritis should not be a generic sheet of ten exercises that everyone gets. It should start with assessment, then match the plan to your symptoms, strength, irritability, goals and available equipment.
Good physiotherapy should help you work out what to load, what to modify, and how to progress without constantly flaring the knee.
A physiotherapy plan may include:
Strength testing and exercise prescription
Gait, stair and squat assessment
Education about flare management
Activity pacing and load planning
Advice about walking, gym, Pilates, cycling or running
Manual therapy as an adjunct where appropriate
Taping or bracing trials in selected cases
A plan for when to progress, hold or reduce load
Manual therapy can be useful for short-term symptom relief in some people, but it should not be the whole plan. In a randomised trial comparing physical therapy with glucocorticoid injection for knee OA, people in the physical therapy group had less pain and functional disability at one year than those receiving glucocorticoid injection (Deyle et al., 2020). That physiotherapy approach included exercise and manual therapy, not passive treatment alone.
Weight management can help when it is relevant
Weight management is not relevant to every person with knee OA, and it should be discussed carefully. But when someone is carrying excess body weight and has symptomatic knee OA, it can be an important part of management.
Even modest weight loss can reduce knee joint load and may improve pain and function for some people with knee OA.
A well-known study by Messier and colleagues found that each pound of body weight lost was associated with about a fourfold reduction in knee joint load per step during walking in overweight and obese older adults with knee OA (Messier et al., 2005).
This does not mean weight is the only issue. It is not. Strong people can have knee OA. Lean people can have knee OA. Pain is not just a maths equation of kilograms through cartilage.
But for some people, combining exercise with nutrition support can be more useful than exercise alone. The key is making the discussion practical, respectful and matched to the person’s goals.
Braces, orthotics and taping may help some people
Braces, orthotics and taping sit in the “may help selected people” category. They are not magic, but they can be useful as part of a broader plan.
Supportive devices can sometimes reduce symptoms enough to help you keep moving while strength and capacity improve.
Options may include:
Unloader braces: sometimes used for medial compartment knee OA
Patellofemoral braces or taping: sometimes useful when pain is mostly around the front of the knee
Foot orthotics: occasionally helpful when foot mechanics appear to contribute to symptoms
Walking poles: useful for hills, hiking or flare periods
Appropriate footwear: helpful for comfort, confidence and walking tolerance
I usually think of these as tools, not cures. If a brace lets you walk more comfortably while you build strength, that can be useful. If it becomes the whole plan, something is missing.
Injections and medication are not the whole answer
Medication decisions sit with your GP or medical specialist, but it is worth understanding where they fit. Pain relief may help some people stay active, sleep better, or manage a flare. That can be useful.
Pain relief may help you participate in rehab, but it does not replace the need to build strength and load tolerance.
The OARSI guideline strongly recommends topical NSAIDs for people with knee OA, while other medication and injection recommendations vary depending on the person’s health profile and OA pattern (Bannuru et al., 2019). This is one reason medication advice should be individualised.
Corticosteroid injections may provide short-term symptom relief for some people. They are not usually a long-term standalone strategy. If an injection reduces pain but the person returns to the same strength deficits, same walking load, and same flare cycle, the underlying capacity problem remains.
Supplements are less convincing than the marketing suggests
Glucosamine and chondroitin are probably the best-known supplements for knee OA. Some people feel they help, and if someone has discussed them with their doctor and wants to continue, that is their decision.
The evidence for glucosamine and chondroitin is much less impressive than the marketing usually sounds.
A BMJ network meta-analysis concluded that glucosamine, chondroitin, or their combination did not reduce joint pain or affect joint space narrowing compared with placebo in people with hip or knee OA (Wandel et al., 2010).
That does not mean every person who takes them is wrong. It means they should not be the main strategy, especially if exercise, strength, pacing and weight management where relevant have not been properly addressed.
Passive treatments alone are not enough
Massage, heat packs, TENS, dry needling and other passive treatments may provide short-term relief for some people. I am not against symptom relief. Pain is exhausting, and if something safe helps you settle a flare, that can be useful.
The problem is when passive treatment becomes the entire plan.
If a treatment makes the knee feel better for a day but does not improve what the knee can tolerate, it is not solving the bigger problem.
Knee OA usually needs an active plan. That means building capacity, improving confidence, and learning how to manage flare-ups rather than relying only on someone else to calm the knee down every few weeks.
When surgery becomes the right conversation
Total knee replacement can be an appropriate and effective option for some people with advanced knee OA, particularly when pain and loss of function remain substantial despite a genuine trial of non-surgical care.
Surgery is not a failure, but it should usually be considered after the non-surgical options have been properly explored.
A randomised controlled trial found that total knee replacement followed by non-surgical treatment produced greater pain relief and functional improvement at 12 months than non-surgical treatment alone in people with moderate to severe knee OA who were eligible for surgery, although both groups improved and surgery carried more adverse events (Skou et al., 2015).
That is the honest position. Some people do very well with non-surgical management. Some people use it to delay surgery. Some people use it to prepare better for surgery. Some people ultimately still need a knee replacement.
The decision should be based on symptoms, function, goals, health status and shared decision-making, not the X-ray wording alone.
If surgery has already been mentioned, this article may help: Can physiotherapy delay knee surgery?
What a sensible non-surgical plan looks like
A good non-surgical plan is not a single treatment. It is a sequence.
The right plan should help you understand your knee, reduce flare cycles, build strength, and keep doing the activities that matter to you where possible.
For many people, that sequence looks like:
Confirm the diagnosis and rule out other causes
Identify the main flare triggers
Set an exercise starting point
Build quadriceps, hip and calf strength
Add aerobic activity at a tolerable level
Modify walking, stairs, hills or gym load temporarily
Use bracing, taping or medication advice where appropriate
Progress toward the activities that matter most
This is not glamorous. It is not a quick fix. But it is the part of knee OA care that has the most consistent support across clinical guidelines.
When to book an in-person assessment
If you have been diagnosed with knee OA and still do not know what to do next, that is a good reason to book an assessment. The same applies if you have been told your knee is “bone on bone”, but no one has explained what you can still improve.
Non-surgical treatment for knee osteoarthritis works best when it is matched to your knee, your symptoms and your goals.
You may benefit from an assessment if:
You have knee OA but no clear plan
You are avoiding stairs, hills, walking or exercise
Your knee keeps flaring after activity
You are unsure which exercises are safe
You have been told surgery may be needed but want to understand your options first
You want a structured plan rather than a generic handout
If you are based in Melbourne’s inner east, including Camberwell, Hawthorn, Kew, Canterbury, Surrey Hills, Glen Iris or nearby, you can book an in-person knee assessment with me at The Hip and Knee Physio.
Emma
References
Australian Commission on Safety and Quality in Health Care. (2024). Osteoarthritis of the knee clinical care standard. ACSQHC. https://www.safetyandquality.gov.au/standards/clinical-care-standards/osteoarthritis-knee-clinical-care-standard
Bannuru, R. R., Osani, M. C., Vaysbrot, E. E., Arden, N. K., Bennell, K., Bierma-Zeinstra, S. M. A., Kraus, V. B., Lohmander, L. S., Abbott, J. H., Bhandari, M., Blanco, F. J., Espinosa, R., Haugen, I. K., Lin, J., Mandl, L. A., Moilanen, E., Nakamura, N., Snyder-Mackler, L., Trojian, T., … McAlindon, T. E. (2019). OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthritis and Cartilage, 27(11), 1578–1589. https://doi.org/10.1016/j.joca.2019.06.011
Bedson, J., & Croft, P. R. (2008). The discordance between clinical and radiographic knee osteoarthritis: A systematic search and summary of the literature. BMC Musculoskeletal Disorders, 9, 116. https://doi.org/10.1186/1471-2474-9-116
Deyle, G. D., Allen, C. S., Allison, S. C., Gill, N. W., Hando, B. R., Petersen, E. J., Dusenberry, D. I., & Rhon, D. I. (2020). Physical therapy versus glucocorticoid injection for osteoarthritis of the knee. New England Journal of Medicine, 382(15), 1420–1429. https://doi.org/10.1056/NEJMoa1905877
Finan, P. H., Buenaver, L. F., Bounds, S. C., Hussain, S., Park, R. J., Haque, U. J., Campbell, C. M., Haythornthwaite, J. A., & Smith, M. T. (2013). Discordance between pain and radiographic severity in knee osteoarthritis: Findings from quantitative sensory testing of central sensitization. Arthritis & Rheumatism, 65(2), 363–372. https://doi.org/10.1002/art.34646
Fransen, M., McConnell, S., Harmer, A. R., Van der Esch, M., Simic, M., & Bennell, K. L. (2015). Exercise for osteoarthritis of the knee: A Cochrane systematic review. British Journal of Sports Medicine, 49(24), 1554–1557. https://doi.org/10.1136/bjsports-2015-095424
Kolasinski, S. L., Neogi, T., Hochberg, M. C., Oatis, C., Guyatt, G., Block, J., Callahan, L., Copenhaver, C., Dodge, C., Felson, D., Gellar, K., Harvey, W. F., Hawker, G., Herzig, E., Kwoh, C. K., Nelson, A. E., Samuels, J., Scanzello, C., White, D., … Reston, J. (2020). 2019 American College of Rheumatology/Arthritis Foundation guideline for the management of osteoarthritis of the hand, hip, and knee. Arthritis & Rheumatology, 72(2), 220–233. https://doi.org/10.1002/art.41142
Messier, S. P., Gutekunst, D. J., Davis, C., & DeVita, P. (2005). Weight loss reduces knee-joint loads in overweight and obese older adults with knee osteoarthritis. Arthritis & Rheumatism, 52(7), 2026–2032. https://doi.org/10.1002/art.21139
Skou, S. T., Roos, E. M., Laursen, M. B., Rathleff, M. S., Arendt-Nielsen, L., Simonsen, O., & Rasmussen, S. (2015). A randomized, controlled trial of total knee replacement. New England Journal of Medicine, 373(17), 1597–1606. https://doi.org/10.1056/NEJMoa1505467
Wandel, S., Jüni, P., Tendal, B., Nüesch, E., Villiger, P. M., Welton, N. J., Reichenbach, S., & Trelle, S. (2010). Effects of glucosamine, chondroitin, or placebo in patients with osteoarthritis of hip or knee: Network meta-analysis. BMJ, 341, c4675. https://doi.org/10.1136/bmj.c4675
Yan, L., Liu, Z., Wang, J., Yuan, W., Wang, Y., Hu, L., & Zeng, C. (2025). Comparative efficacy and safety of exercise modalities in knee osteoarthritis: Systematic review and network meta-analysis. BMJ, 391, e085242. https://doi.org/10.1136/bmj-2025-085242
Medical disclaimer
This blog is general educational information only and is not a substitute for individual medical advice, diagnosis or treatment. If you have severe or worsening knee pain, a hot or rapidly swollen joint, fever, recent trauma, inability to weight-bear, significant locking, new neurological symptoms, calf swelling, shortness of breath, or symptoms that concern you, please seek medical review promptly.


Comments