
Knee Osteoarthritis Symptoms: Early Signs of Knee Arthritis
- Emma Glynn
- Jun 8
- 10 min read

By Emma Glynn - The Hip & Knee Physio
If you have started noticing knee arthritis symptoms, it may not feel dramatic at first. The early symptoms of knee arthritis can be subtle: stiffness in the morning, aching after a longer walk, swelling that comes and goes, or discomfort with stairs, hills, squats or getting out of a low chair.
Many people describe this as “just getting older”, but that phrase is not very useful. It does not tell you what is happening, what is safe to keep doing, or when it is worth getting proper advice. It can also make people ignore symptoms for too long, or worry unnecessarily because an X-ray used words like “degenerative change”.
Knee osteoarthritis is common, but it does not mean your knee is useless, fragile, or beyond help.
I am Emma Glynn, an APA Titled Musculoskeletal Physiotherapist in Camberwell. I work exclusively with hip and knee conditions, and I often assess active adults over 45 who want to keep walking, exercising, travelling, running, playing golf, or simply moving with more confidence.
For a broader overview of assessment and treatment options, you can visit my knee osteoarthritis page.
What knee osteoarthritis means
Knee osteoarthritis, often shortened to knee OA, is a condition that affects the whole knee joint. It is not just “worn cartilage”. The joint lining, bone, cartilage, ligaments, menisci, muscles and nervous system can all contribute to how the knee feels and functions.
The phrase “wear and tear” is common, but I do not love it. It makes the knee sound like a car tyre that has run out of tread. Human joints are more adaptable than that.
Knee OA is better understood as a whole-joint condition where symptoms are influenced by load, strength, inflammation, sensitivity, general health and activity patterns.
In Australia, osteoarthritis is the most common form of arthritis, with around 2.1 million Australians estimated to be living with osteoarthritis based on 2022 National Health Survey data (Australian Institute of Health and Welfare, 2024). It becomes more common with age, but age alone does not tell the whole story.
Previous knee injury, body weight, genetics, muscle strength, occupational load, sport history and general physical health can all influence risk and symptoms.
Early symptoms of knee arthritis often start gradually
The early symptoms of knee arthritis are usually subtle. Many people do not wake up one morning with a dramatically painful knee. More often, they notice small changes that slowly become harder to ignore.
Early symptoms of knee arthritis often show up as stiffness, aching, swelling, or reduced confidence with loaded activities such as stairs, hills and squatting.
Common knee osteoarthritis symptoms include:
Aching pain around the knee joint
Morning stiffness that eases once you get moving
Pain after longer walks, stairs, hills or gardening
Difficulty getting out of low chairs
Pain or stiffness after sitting for a while
Swelling that comes and goes
Grinding, clicking or creaking
Good days and bad days
Reduced confidence kneeling, squatting or walking downhill
These symptoms can overlap with other knee problems, which is why the pattern matters.
If your knee symptoms started around your mid-40s or later and have become more noticeable over time, this article on knee arthritis after 45 may help you understand the pattern more clearly.
Knee arthritis symptoms often feel achy rather than sharp
Knee OA pain is often described as a dull ache, heaviness, pressure, or soreness around the joint. It may sit around the inside of the knee, outside of the knee, behind the kneecap, or deeper within the joint.
Some people feel it more after activity. Others feel stiff and sore when they first get up, then better once they are moving.
A common knee arthritis symptom pattern is pain that builds with load and settles with relative rest.
That does not mean every ache is osteoarthritis. Sharp catching, true locking, sudden swelling after injury, or marked instability may suggest another issue, such as a meniscus injury, ligament injury, inflammatory condition, or acute flare that needs a different assessment.
The important thing is not just where the pain is, but how it behaves.
Morning stiffness is a common clue
Morning stiffness is one of the more recognisable knee osteoarthritis symptoms. The knee may feel thick, tight, swollen, rusty or reluctant when you first get out of bed.
In typical knee OA, this stiffness usually eases once you get moving. NICE guidance describes clinical OA as more likely in people aged 45 or over who have activity-related joint pain and either no morning stiffness or morning stiffness lasting no longer than 30 minutes (National Institute for Health and Care Excellence, 2022).
If your knee stiffness eases within about 30 minutes, that pattern can fit osteoarthritis, but prolonged morning stiffness may need a different medical review.
Longer-lasting stiffness, especially if it affects multiple joints or comes with marked warmth, redness, fatigue or systemic symptoms, may suggest an inflammatory arthritis picture rather than straightforward knee OA.
Stairs, hills and low chairs often expose knee OA
Stairs are a classic complaint. Many people with knee OA notice that going downstairs is harder than going upstairs. This is partly because descending stairs places a higher demand on the quadriceps and front of the knee.
Low chairs, deep couches, toilets, squatting, kneeling, hills and uneven ground can also become more noticeable.
Knee OA often shows itself when the knee is asked to control load, not just when it is sitting still.
This is why symptoms can feel confusing. You might be fine walking around the house, then sore after a long shopping trip. You might manage flat walking, but flare on hills. You might feel good during exercise, then stiffen later that day or the next morning.
That pattern does not mean you have “damaged” the knee each time it hurts. It often means the knee has exceeded its current load tolerance.
Swelling can come and go
Some people with knee OA notice intermittent swelling. The knee may look puffy, feel full, or become harder to bend after a busy day. This can happen when the joint lining becomes irritated and produces more fluid.
Swelling that comes and goes after activity can occur with knee OA, but a hot, rapidly swollen or severely painful joint should be assessed promptly.
You should seek medical review if swelling is:
Sudden and severe
Hot, red or associated with fever
Linked to a fall or injury
Associated with inability to weight-bear
Accompanied by significant calf pain or unexplained shortness of breath
Not settling or progressively worsening
Not all swelling is dangerous, but the behaviour of the swelling matters.
Clicking and grinding do not always mean damage
Knee noises can be unnerving. Grinding, clicking, crunching and creaking can make people feel as if the joint is crumbling. Sometimes crepitus, the medical term for joint noise or grating, occurs with knee OA. Sometimes it occurs in people without major symptoms.
A knee-OA-specific study found that people with knee OA and crepitus had slightly lower self-reported physical function and knee-related quality of life, but crepitus was not associated with objective function or knee strength (Pazzinatto et al., 2019).
Knee noise matters more when it comes with pain, swelling, locking, giving way or loss of function.
A noisy knee by itself is not a reason to stop moving. In fact, becoming fearful of safe movement can be more limiting than the noise itself.
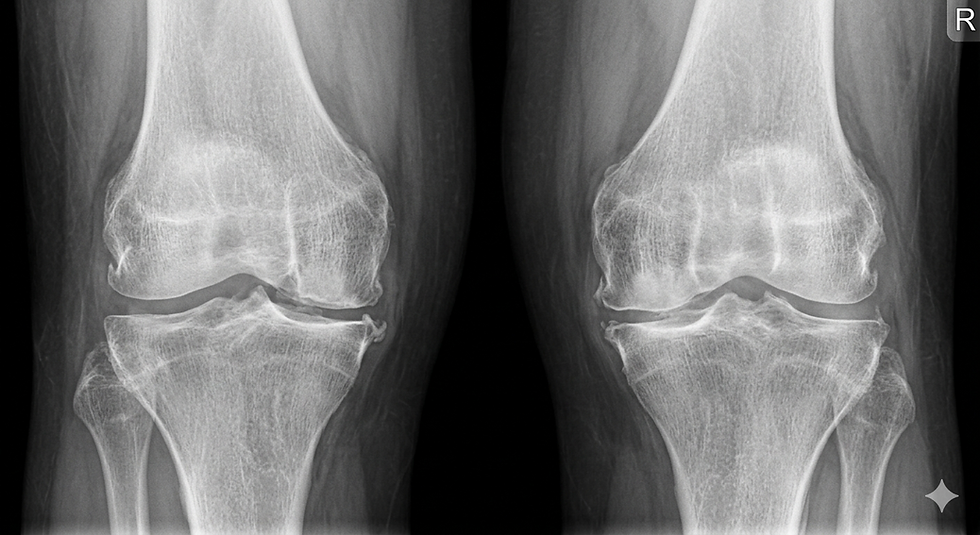
The X-ray does not tell the whole story
This is one of the most important things I explain to patients. An X-ray can show structural changes, but it does not perfectly predict pain or function.
Some people have significant X-ray changes and surprisingly manageable symptoms. Others have mild X-ray findings but quite limiting pain. Research has consistently shown discordance between radiographic OA and symptoms in many people (Bedson & Croft, 2008; Finan et al., 2013).
Your symptoms, strength, function and goals matter more than the wording on the scan report alone.
NICE recommends that imaging is not routinely needed to diagnose osteoarthritis when the clinical presentation is typical, unless there are atypical features or signs of another diagnosis (National Institute for Health and Care Excellence, 2022). The Australian Osteoarthritis of the Knee Clinical Care Standard also emphasises timely assessment, education, exercise, weight management where relevant, and appropriate non-surgical care before surgery is considered (Australian Commission on Safety and Quality in Health Care, 2024).
So if your report says “mild degenerative change”, that does not mean your pain is imaginary. If it says “bone-on-bone”, that does not automatically mean surgery is the only option. The clinical picture matters.
What knee osteoarthritis symptoms do not usually look like
It is helpful to know when symptoms do not sound like typical knee OA. This does not mean you need to panic. It means the knee may need a different assessment pathway.
Symptoms that are sudden, severe, inflammatory, traumatic or neurological should not be brushed off as simple osteoarthritis.
Knee OA is less likely to be the only explanation if you have:
Sudden severe pain after a clear injury
True locking where the knee cannot straighten
Rapid, hot, red swelling without an obvious reason
Fever or feeling generally unwell with a swollen joint
Marked instability or repeated giving way
New numbness, weakness or referred pain from the back
Severe night pain that is not position-related
Unexplained weight loss or systemic symptoms
If any of these apply, you should seek assessment from a GP, physiotherapist or appropriate medical professional.
Can you keep exercising with knee OA?
In many cases, yes. Exercise is one of the best-supported first-line treatments for knee OA. The goal is not to punish the knee or ignore symptoms. The goal is to find the right dose of movement and strength work for your current capacity.
For most people with knee OA, the question is not whether to move, but how to move in a way the knee can tolerate and adapt to.
Exercise for knee OA may include:
Strength training
Walking or cycling
Water-based exercise
Balance and neuromuscular work
Mobility exercises
Gradual return to valued activities
The American College of Rheumatology and Arthritis Foundation strongly recommend exercise for knee OA, with options including walking, strengthening, neuromuscular training and aquatic exercise (Kolasinski et al., 2020). A 2025 systematic review and network meta-analysis also found that different exercise modalities can improve pain, function, gait performance and quality of life in people with knee OA, with aerobic exercise ranking highly across several outcomes (Yan et al., 2025).
If you are wondering whether you can keep running, I have written more here: Can you keep running with knee osteoarthritis?
Common questions about knee arthritis symptoms
What are the first signs of knee arthritis?
The first signs of knee arthritis often include morning stiffness, aching after activity, pain with stairs or hills, swelling that comes and goes, and reduced confidence with squatting or getting out of low chairs.
The early symptoms are often more about stiffness, load sensitivity and fluctuating function than constant severe pain.
Does knee osteoarthritis always show on an X-ray?
Not always in a way that matches symptoms. Some people have X-ray changes with little pain, while others have significant pain with only mild imaging changes.
An X-ray can be useful in some situations, but it does not replace a proper assessment of symptoms, strength and function.
Can knee osteoarthritis symptoms come and go?
Yes. Knee OA symptoms often fluctuate. Many people have good days, flare-ups, and periods where symptoms settle again.
Good days and bad days are common in knee OA, which is why pacing and load planning matter.
When should I get knee arthritis symptoms checked?
It is worth getting assessed if knee pain or stiffness lasts more than a few weeks, changes how you walk or exercise, affects stairs, or leaves you unsure what activity is safe.
The right time to get assessed is often when symptoms start changing what you do, not when you have already stopped doing everything.
When it is worth getting assessed
You do not need to wait until your knee is unbearable before getting help. Assessment can be useful when symptoms are starting to change your behaviour.
It is worth getting assessed when knee symptoms start making decisions for you.
That might look like:
Avoiding stairs
Shortening your walks
Stopping gym, Pilates or running
Feeling nervous about hills or uneven ground
Needing longer to warm up in the morning
Having repeated flares after activity
Being told you have OA but not being given a plan
Feeling unsure which exercises are safe
A good physiotherapy assessment should help clarify whether your symptoms fit knee OA, whether another diagnosis needs to be considered, and what the next step should be.
If surgery has already been mentioned, this article explains what physiotherapy can offer before knee surgery is considered.
What happens after diagnosis?
Knee OA is not something you simply ignore until it becomes “bad enough”. It is a condition that can often be managed with a structured plan.
Current best-practice care usually includes education, exercise, physical activity advice, weight management support where relevant, and strategies to manage flare-ups. Medication, injections or surgical referral may be relevant in some cases, but they are not the first or only options for everyone.
The aim is to improve what your knee can tolerate, reduce unnecessary flare cycles, and help you stay active in a way that makes sense for your life.
If you are based in Melbourne’s inner east, including Camberwell, Hawthorn, Kew, Canterbury, Surrey Hills, Glen Iris or nearby, you can book an in-person knee assessment with me at The Hip and Knee Physio.
Emma
References
Australian Commission on Safety and Quality in Health Care. (2024). Osteoarthritis of the knee clinical care standard. ACSQHC. https://www.safetyandquality.gov.au/standards/clinical-care-standards/osteoarthritis-knee-clinical-care-standard
Australian Institute of Health and Welfare. (2024). Osteoarthritis. AIHW. https://www.aihw.gov.au/reports/chronic-musculoskeletal-conditions/osteoarthritis
Bedson, J., & Croft, P. R. (2008). The discordance between clinical and radiographic knee osteoarthritis: A systematic search and summary of the literature. BMC Musculoskeletal Disorders, 9, 116. https://doi.org/10.1186/1471-2474-9-116
Finan, P. H., Buenaver, L. F., Bounds, S. C., Hussain, S., Park, R. J., Haque, U. J., Campbell, C. M., Haythornthwaite, J. A., & Smith, M. T. (2013). Discordance between pain and radiographic severity in knee osteoarthritis: Findings from quantitative sensory testing of central sensitization. Arthritis & Rheumatism, 65(2), 363–372. https://doi.org/10.1002/art.34646
Kolasinski, S. L., Neogi, T., Hochberg, M. C., Oatis, C., Guyatt, G., Block, J., Callahan, L., Copenhaver, C., Dodge, C., Felson, D., Gellar, K., Harvey, W. F., Hawker, G., Herzig, E., Kwoh, C. K., Nelson, A. E., Samuels, J., Scanzello, C., White, D., … Reston, J. (2020). 2019 American College of Rheumatology/Arthritis Foundation guideline for the management of osteoarthritis of the hand, hip, and knee. Arthritis Care & Research, 72(2), 149–162. https://doi.org/10.1002/acr.24131
National Institute for Health and Care Excellence. (2022). Osteoarthritis in over 16s: Diagnosis and management (NICE guideline NG226). NICE. https://www.nice.org.uk/guidance/ng226
Pazzinatto, M. F., de Oliveira Silva, D., Barton, C. J., & Ferreira, A. S. (2019). What are the clinical implications of knee crepitus to individuals with knee osteoarthritis? An observational study with data from the Osteoarthritis Initiative. Brazilian Journal of Physical Therapy, 23(6), 491–496. https://doi.org/10.1016/j.bjpt.2018.11.001
Yan, L., Liu, Z., Wang, J., Yuan, W., Wang, Y., Hu, L., & Zeng, C. (2025). Comparative efficacy and safety of exercise modalities in knee osteoarthritis: Systematic review and network meta-analysis. BMJ, 391, e085242. https://doi.org/10.1136/bmj-2025-085242
Medical disclaimer
This blog is general educational information only and is not a substitute for individual medical advice, diagnosis or treatment. If you have severe or worsening knee pain, a hot or rapidly swollen joint, fever, recent trauma, inability to weight-bear, significant locking, new neurological symptoms, or symptoms that concern you, please seek medical review promptly.



Comments